I want to thank Veronica Vargas for sending me the following link from the Institute for Health Metrics and Evaluation (IHME) , which features innovative ways of displaying different cuts of US and international data from a massive data files. Viewing this site will perhaps take you fifteen minutes or more to get a feel. It is staffed by the University of Washington, but appears to be funded largely by the Gates Foundation. It has been around for a while, but they are making a big push on its features this fall.
The first link decomposes spending in the US by disease, by broad type of service (pharmacy, IP, OP, Dentist, ER).
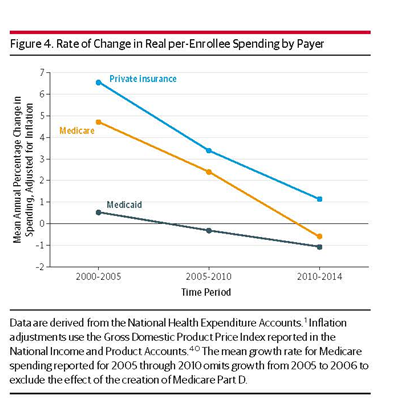
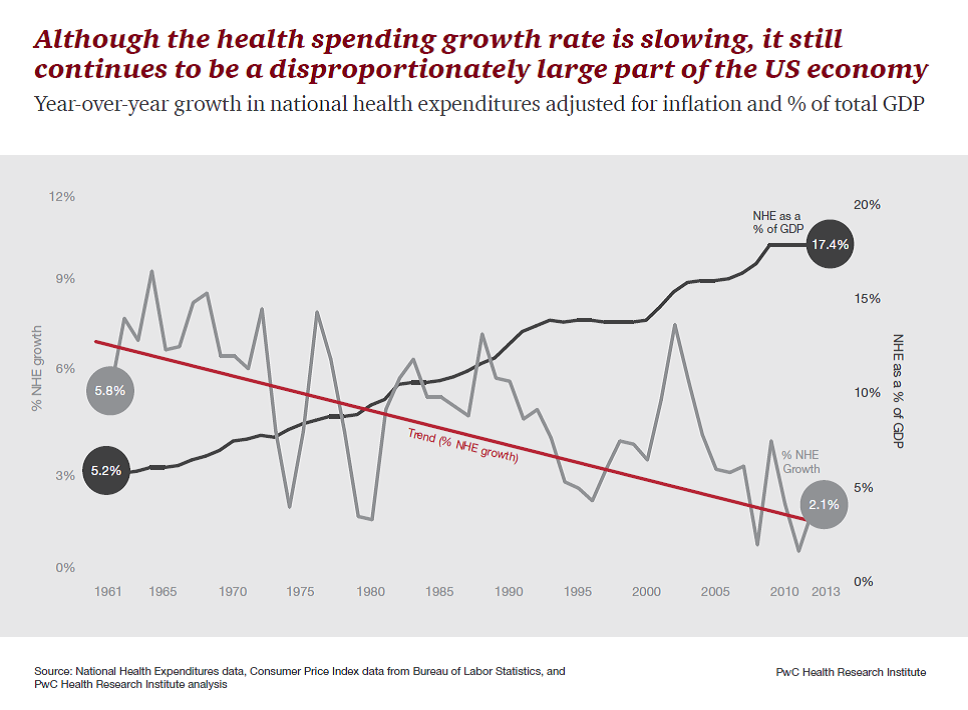
They document the well-known result that about half of the US increase is due to price increases, not intensity or illness, although aging and pop growth contribute.US costs are higher than the rest of the world largely because our prices paid for all types of care are much higher than elsewhere. And increasingly so.
Here is a direct link to the interesting interactive figures. Try the four different tabs across the top if you are curious. (Is a little slow on my wireless laptop.)
https://vizhub.healthdata.org/dex/
It allows you to drill down to questions such as how much was spent on individual disease for certain ages, on emergency department.
If you click on “visualizations“ in the upper right, you get different views that can be plotted, which are very extensive.
Or start here http://www.healthdata.org/results/data-visualizations
Below is a link to the article originally posted, along with a sample figure.
Factors associated with increases in US health care spending, 1996–2013
Here is one that lets you choose one or compare two or more countries disease burdens along multiple dimensions.
https://vizhub.healthdata.org/gbd-compare/
The say that their mission includes sharing data for researchers. Here is a link to various data that they support and document with a nice search tool.
http://ghdx.healthdata.org/data-by-type
Global Burden of Disease module lets you answer questions as specific as how many people die of air pollution in India in 2013.
Here is how they describe it.
September 14, 2017
Data Visualization
Analyze updated data about the world’s health levels and trends from 1990 to 2016 in this interactive tool. Use treemaps, maps, arrow diagrams, and other charts to compare causes and risks within a country, compare countries with regions or the world, and explore patterns and trends by country, age, and gender. Drill from a global view into specific details. Compare expected and observed trends. Watch how disease patterns have changed over time. See which causes of death and disability are having more impact and which are waning.
This is not a site oriented toward hypothesis testing, although it does include confidence intervals on many estimates (which seem to only reflect sampling precision, not other sources of uncertainty such as the quality of the underlying data.) For me, the main use will be in writing in the introduction of a paper so as to summarize how large a problem is, or how many people have a given condition, or how it is growing etc. The international breadth is stunning. At a different level, it is a good example of how big data can be manipulated using “cubes” and different cuts of the data to show fascinating patterns (girls less than 1 year cost $11,000 each on average, which drops to $1,600 age 5-9, and it is not until age 65 in the US that female mean cost is again over $11,000. It peaks at $31,000 per year over age 85.)
Be forewarned: you can spend a lot of time playing around…